
Introduction
Running related injuries (RRI’s) are common in long distance runners with injury incidence shown to range between 17.8 (95% CI 16.7-19.1) injuries per 1000 hours of running in novice runners and 7.7 (95% CI 6.9-8.7) injuries per 1000 hours of running in recreational runners.[1] Known risk factors for RRI’s include history of previous injury and a greater training distance per week while a gradual increase in training distance per week is a protective factor. [2]
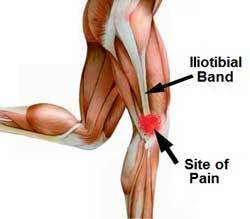
ITB Syndrome Anatomy
Cause
Iliotibial band syndrome (ITBS) is the second most common RRI and the most common cause of lateral knee pain in runners.[3] The aetiology of ITBS is thought to be multifactorial and remains poorly understood however several biomechanical risk factors have been proposed to contribute to the condition.[4] Traditionally, ITBS was thought to be caused by friction or excessive pressure at the distal iliotibial band (ITB) as it passes over the lateral femoral epicondyle during repetitive knee flexion and extension. [5] A more recent theory suggests that impingement at this site contributes to the condition rather than purely excessive lateral pressure.[6, 7]
Biomechanical Risk Factors
Proposed biomechanical risk factors for ITBFS include increased peak hip adduction,[8] knee internal rotation,[8-10] peak trunk ipsilateral flexion,[10, 11] and peak rearfoot pronation[12] as these factors can increase abnormal lengthening of the ITB (i.e. excess strain) and contribute to compression of the ITB at the lateral femoral condyle (i.e. excess stress).[13]
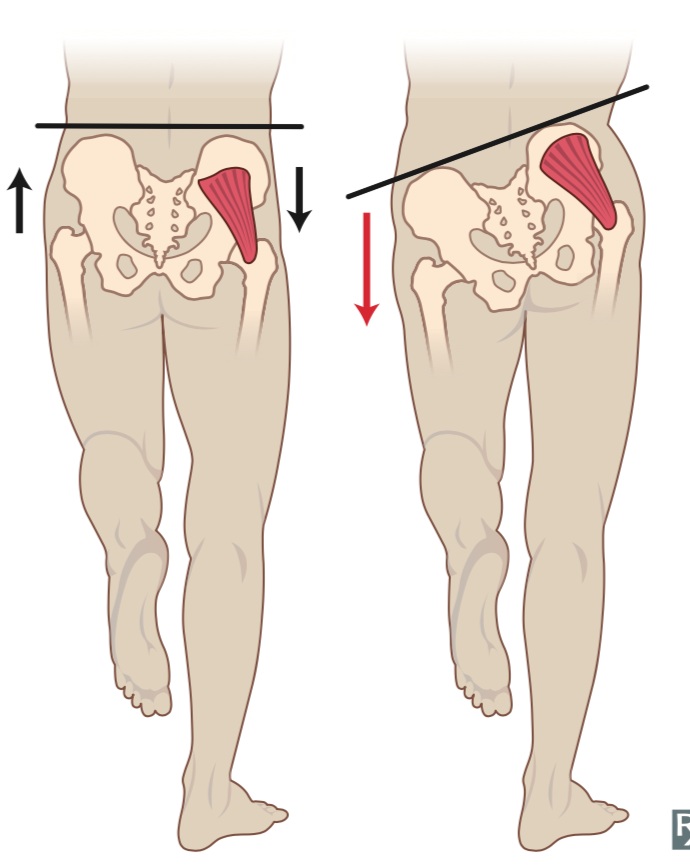
Poor Biomechanincs (Right) can contribute to ITBS
Prevention and Management
Preventative measures for ITBFS should include an appropriate training plan that includes gradual increases in running distance and appropriate load management strategies including programmed rest days and de-load phases.[2]
Management
The acute management of ITBS should focus on anti-inflammatory modalities, relative rest, soft tissue release and addressing biomechanical factors known to contribute to ITBS.[13] As irritability settles running can be gradually re introduced in line with a periodised running plan. Running retraining incorporating running with an increased cadence has been shown to increase the gluteal muscle recruitment during foot strike and mid stance of the running cycle [14] and may help to decrease load at the ITB insertion in patients with ITBS.
There is debate as to whether it is possible to modify running mechanics with strengthening exercises alone however positive results have been demonstrated in studies that focus on isometric and eccentric strength of the glute muscles in running specific positions[15] and include visual feedback with cueing.[16] The hip abductor muscles are known to contribute to peak hip adduction, knee internal rotation, ipsilateral trunk flexion[17] and have been shown to be related to other lower limb RRI’s.[14] Two gluteal muscles that control frontal and transverse plane hip and pelvic motion during running include the glute max and glute med.[14] Glute max EMG is shown to be highest in the step up and single leg squat exercise while the glute med EMG is shown to be highest in the side bridge with hip abduction exercise [18] (See Pictures Below). Despite a lack of prospective research it is plausible to include gluteal strengthening 2-3 x per week in the management of ITBS given the gluteal muscles’ relationship to biomechanical factors known to be associated with the condition.
While foot and ankle orthosis have been proposed as a tool to maintain a neutral foot position and control tibial internal rotation during running[19] to date, no prospective studies have investigated the use of orthosis for patients with ITBS.

Single Leg Squat

Side Bridge with Hip Abduction
Conclusion
Based off the available evidence the best management for ITBS includes appropriate management in the acute stage to settle irritability followed by gluteal strengthening with an emphasis on isometric and eccentric frontal and transverse plane movements and physiotherapist guided running retraining.
Take Away Points
· ITBS is the second most common RRI and the most common cause of lateral knee pain in runners.
· ITBS is thought to be caused by either excessive lateral pressure or impingement as the ITB runs over the lateral femoral epicondyle during knee flexion and extension.
· Gluteal weakness is proposed as a modifiable contributing factor in ITBS.
· Gluteal strengthening should focus on isometric and eccentric exercises in running specific positions and should be carried out with appropriate cueing and visual feedback.
· Running retraining including running with an increased cadence has been proposed to increase gluteal muscle activation during running.
Written by Cameron Dyer – Physiotherapist and Athlete Rehab Specialist
References
1. Videbæk, S., et al., Incidence of Running-Related Injuries Per 1000 h of running in Different Types of Runners: A Systematic Review and Meta-Analysis. Sports Medicine, 2015. 45(7): p. 1017-1026.
2. van Gent, R.N., et al., Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. British Journal of Sports Medicine, 2007. 41(8): p. 469-480.
3. Taunton, J.E., et al., A retrospective case-control analysis of 2002 running injuries. British Journal of Sports Medicine, 2002. 36(2): p. 95.
4. Beers, A., et al., Effects of Multi-modal Physiotherapy, Including Hip Abductor Strengthening, in Patients with Iliotibial Band Friction Syndrome. Physiotherapy Canada. Physiotherapie Canada, 2008. 60(2): p. 180-188.
5. Orchard, J.W., et al., Biomechanics of Iliotibial Band Friction Syndrome in Runners. The American Journal of Sports Medicine, 1996. 24(3): p. 375-379.
6. Hamill, J., et al., A prospective study of iliotibial band strain in runners. Clinical Biomechanics, 2008. 23(8): p. 1018-1025.
7. Fairclough, J., et al., Is iliotibial band syndrome really a friction syndrome? Journal of Science and Medicine in Sport, 2007. 10(2): p. 74-76.
8. Noehren, B., I. Davis, and J. Hamill, ASB clinical biomechanics award winner 2006 prospective study of the biomechanical factors associated with iliotibial band syndrome. Clinical biomechanics (Bristol, Avon), 2007. 22(9): p. 951.
9. Ferber, R., et al., Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. The Journal of orthopaedic and sports physical therapy, 2010. 40(2): p. 52.
10. Foch, E., et al., Associations between iliotibial band injury status and running biomechanics in women. Gait & Posture, 2015. 41(2): p. 706-710.
11. Foch, E. and C.E. Milner, The influence of iliotibial band syndrome history on running biomechanics examined via principal components analysis. Journal of Biomechanics, 2014. 47(1): p. 81-86.
12. Messier, P.S., et al., Etiology of iliotibial band friction syndrome in distance runners. Medicine & Science in Sports & Exercise, 1995. 27(7): p. 951-960.
13. Baker, R.L. and M. Fredericson, Iliotibial Band Syndrome in Runners: Biomechanical Implications and Exercise Interventions: Biomechanical Implications and Exercise Interventions. Physical Medicine & Rehabilitation Clinics of North America, 2016. 27(1): p. 53-77.
14. Semciw, A., R. Neate, and T. Pizzari, Running related gluteus medius function in health and injury: A systematic review with meta-analysis. Journal of Electromyography and Kinesiology, 2016. 30: p. 98-110.
15. Fredericson, L.M., et al., Hip Abductor Weakness in Distance Runners with Iliotibial Band Syndrome. Clinical Journal of Sport Medicine, 2000. 10(3): p. 169-175.
16. Barrios, J.A., K.M. Crossley, and I.S. Davis, Gait retraining to reduce the knee adduction moment through real-time visual feedback of dynamic knee alignment. Journal of Biomechanics, 2010. 43(11): p. 2208-2213.
17. Mucha, M.D., et al., Hip abductor strength and lower extremity running related injury in distance runners: A systematic review. Journal of Science and Medicine in Sport, 2017. 20(4): p. 349-355.
18. Macadam, P., J. Cronin, and B. Contreras, An examination of the gluteal muscle activity associated with dynamic hip abduction and hip external rotation exercises. A systematic review. International journal of sports physical therapy, 2015. 10(5): p. 573.
19.Aderem, J. and Q.A. Louw, Biomechanical risk factors associated with iliotibial band syndrome in runners: A systematic review Rehabilitation, physical therapy and occupational health. BMC Musculoskeletal Disorders, 2015. 16(1): p. <xocs:firstpage xmlns:xocs=""/>.