Low back pain in young athletes is more common than you’d think, but one type of injury that should not be missed and diagnosed correctly is lumbar bone stress injuries.
These injuries are sneaky. They can look like everyday back pain but may actually involve stress to the bones in your lower spine, and if missed, they can delay return to sport or even cause long-term problems.
Let’s break it down so you know what to look out for and what to do about it.
What Are Lumbar Bone Stress Injuries?
These injuries affect the posterior elements of the lumbar spine, mainly a region called the pars interarticularis, a small bridge of bone connecting the vertebrae.
You may hear terms like:
Spondylolysis – a stress reaction or fracture in the pars
Spondylolisthesis – when the vertebra slips forward, often due to a pars injury
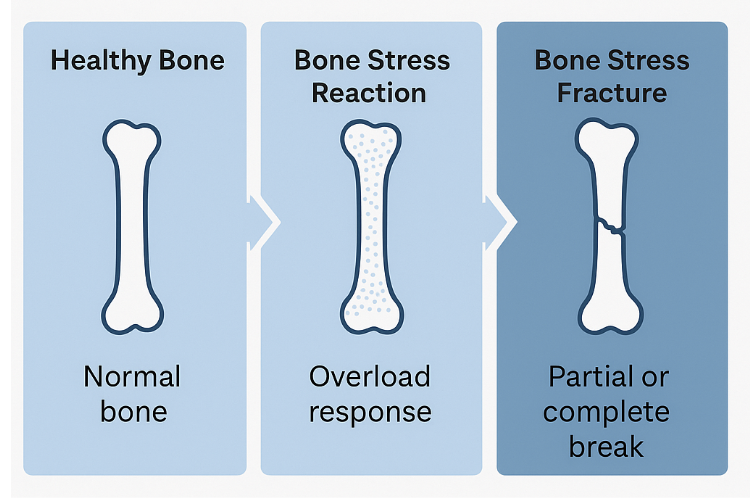
Bone stress reaction/fracture – part of a continuum of overuse injury
Non-uniting stress fracture – a stress fracture that hasn't fully healed within the expected timeframe but shows fibrous healing, indicating biological repair and often remaining stable with appropriate load management.

These injuries are a lot like shin splints; they happen when the bone is overloaded by repeated movements like jumping, twisting, or bending backwards. At first, it’s just tiny stress on the bone, but if the load keeps building without enough rest, it can develop into a stress fracture. They often show up early in the season, during pre-season, or when there’s a sudden increase in training after a break.
t is critical to identify bone stress injuries early because continuing to load an already stressed bone can cause the injury to worsen, potentially progressing from a stress reaction to a full fracture. This not only increases the severity of the injury but also significantly prolongs recovery time, often requiring weeks to months of complete rest from sport. Early detection allows for timely offloading, targeted rehab, and a quicker, safer return to activity.
Who Gets These Injuries?
Lumbar bone stress injuries are most common in:
Teen athletes aged 11-18
Athletes who partake in sports with back extension, rotation or side-bending (e.g. cricket fast bowling, gymnastics, AFL, soccer, tennis)
Athletes who’ve had a sudden spike in training or competition
How Does It Happen?
Repetitive lumbar extension + rotation (e.g., kicking, jumping, arching, throwing)
Sudden increase in training volume or intensity
Poor technique or poor core control
Inadequate recovery between sessions
Over time, the bone fatigues faster than it can repair – that’s when injury happens.
Adolescents are more suceptible during growth sports:
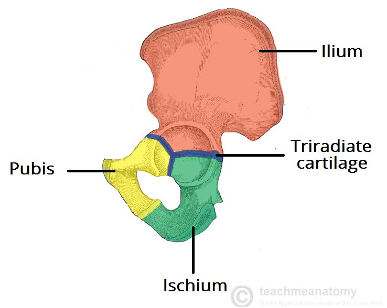
Peak Height Velocity (PHV) is the period during adolescence when growth in height is at its fastest, typically between ages 11–13 in females and 13–15 in males.
During this time, bone mineral density temporarily drops and coordination declines due to rapid skeletal growth outpacing muscular and neuromuscular adaptation. This makes the spine, particularly the lumbar region, more vulnerable to overload and bone stress injuries.
Common Symptoms
What makes lumbar bone stress injuries tricky is that they can feel just like regular low back pain. A physio will look closely at your history, symptoms, and how your back responds to certain movements to decide if a bone stress injury might be the cause.
Symptoms can include:
Localised low back pain (one or both sides)
Worse with arching, bending back, twisting
Tight hamstrings or glutes
Pain with prolonged standing or running
Often, no pain at rest
May feel better after warm-up, worse after activity
Red flags to seek physio/doctor immediately:
Tingling, numbness, or weakness in legs
Night pain or constant, non-resolving pain
Sudden loss of function
What Can It Be Mistaken for?
As we’ve mentioned before, lumbar bone stress can masquerade as other conditions of the low back, including:
Non-specific low back pain
Muscle spasm or strain
Facet joint pain
Sacroiliac joint irritation
That’s why accurate diagnosis matters. If we suspect a lumbar bone stress injury, we’ll refer for an MRI, as X-rays often miss early stress reactions. These early-stage injuries don’t show up well on X-ray because there is no visible fracture line or cortical disruption. X-rays detect changes in bone density and structure, which typically occur later in the injury process. Additionally, lumbar spine X-rays often require oblique views, which expose the athlete to relatively higher doses of radiation. MRI, on the other hand, is more sensitive to early bone marrow changes and doesn’t involve radiation, making it the preferred imaging choice in young athletes.
What Can Physio Do?
If caught early, these injuries heal really well with the right approach. At High-Performance Rehab, we guide you through a structured plan:

Phase 1 – Acute (0–8 weeks)
Rest from aggravating activity (no running, jumping, twisting)
Swelling management & pain relief
Light core control and hip strengthening
Biking for alternative cardio to prevent loss of cardiovascular fitness
Phase 2 – Load Introduction (8–16 weeks)
Guided return to sport-specific drills - Gradually reintroduces mechanical loading to the healing bone in a controlled, progressive way.
Core, glute & lumbar strengthening - Weakness can lead to compensatory loading through the lower limbs, especially at the site of previous BSI.
Movement control retraining - Poor control can result in altered biomechanics (e.g. excessive hip adduction or internal rotation), increasing stress on specific bone sites.
Gradual build-up to training loads
Phase 3 - Strength Accumulation (17+ weeks)
Continue a gym full-body (upper, lower, core) based program
Monitor and maintain training loads
Most athletes return to full sport within 3–4 months, depending on the severity and timing of diagnosis. The earlier a suspected bone stress injury is diagnosed, the earlier we can start the offload process.
Can It Be Prevented?
Yes, and that’s the best part.
Our prevention strategies include:
Gradual increases in training volume (no big spikes)
Regular technique check-ups (especially for bowlers and kickers)
Core and hip stability work
Load monitoring for game + training, and school sports
I.e. As per Play Cricket - Australian Cricket Junior Bowling Guidelines recommends a maximum of 3 bowling days per week (match & training) A maximum of 5 overs in each bowling spell for U13-U17 age groups
Struggling With Back Pain?
Don’t turn the stress reaction into a fracture and be proactive with diagnosis and management.
Book an assessment with one of our physios today. We’ll help uncover the cause and map out a plan to get you back doing what you love, safely and confidently.
Article Written by: Martin Law