
Background
Plantar fasciopathy (previously known as plantar fasciitis) is the most common cause of heel pain in adults and affects up to 8% of running-based athletes. (Taunton et al., 2002) Symptoms of plantar fasciopathy include pain at the base of the heel that is worst in the morning or when performing sporting activity, particularly when warming up. (Thing, 2012) Plantar fasciopathy usually results from an acute overload of the plantar fascia i.e. when commencing a new sport or a chronic overload related to lifestyle and exercise factors. Risk factors for plantar fasciopathy include reduced ankle dorsi flexion, BMI > 30kg/m2 and work-related weight-bearing.(Riddle, Pulisic, Pidcoe, & Johnson, 2003)
Recent evidence suggests that the condition should be referred to as fasciopathy rather than fasciitis as the tissue pathology more closely resembles that of tendinosis. (Drew, Smith, Littlewood, & Sturrock, 2014; Lemont, Ammirati, & Usen, 2003)
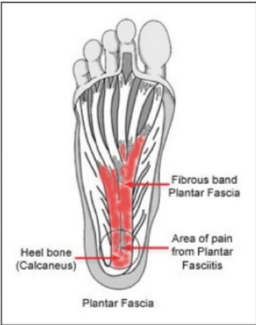
Plantar Fascia Anatomy
Assessment and Diagnosis
Plantar fasciopathy is generally diagnosed clinically however ultrasound can assist if clinical diagnosis is uncertain. Ultrasound can be used to measure the thickness of the fascia however ultrasound findings have not been shown to change despite improvements in outcome. (Rathleff et al., 2015) In some case, patients with plantar fasciopathy present to physiotherapy with an X-Ray that may show a bone spur at the base of the heel. Interestingly, this has not been shown to be related to pain or outcome therefore is generally not of use in guiding management.(Lu, Gu, & Zhu, 1996)
Treatment and Rehabilitation
Treatment of plantar fasciopathy has traditionally consisted of stretching, gel heel inserts and injections (Rathleff & Thorborg, 2015) however recent advances in understanding of the pathology has led to increased focus on exercise and load management as treatment options.
A recent study by Rathleff et al, (2015) showed that a program of slow high-load strength training outperformed a stretching program over 3 months. The strength program consisted of progressively overloading a single leg calf raise performed in toe flexion (Image 1/Image 2) and progressing every second week. It is a high load slow tempo strength program. Stretching consisted of 10 x 10 sec stretches performed 3 x per day.

Start position

End position
The rationale behind the slow high load strength training program is that the program provides a progressive overload of the plantar fascia that promotes collagen synthesis to help normalise tendon structure and improve tissue capacity.(Rathleff et al., 2015)
While other management options do exist and are called in some cases of plantar fasciopathy the mainstay of effective management should be an appropriate load management and strengthening program administered and reviewed regularly by your physiotherapist.
Patient Tips
· Increase the load on the plantar fascia by filling a back pack with books as you get stronger.
· Perform the single leg calf raise with a rolled towel under your toe to utilise the ‘windlass mechanism’ whereby flexing the toes causes tensioning of the plantar fascia prior to loading.
· Manage your activities around your pain threshold i.e. pain > 4/10 during or after loading suggests you have overloaded the tissue. For best results, discuss with your sports physiotherapist about an individualised load management plan.
Clinical Tip
· When treating athletes or patients with plantar fasciopathy treatment outcomes are best measured using the Foot Function Index (FFI). The FFI consists of 23 items divided into three subscales that quantify the impact of foot pathology on pain, disability and activity limitations. Scores range from 0-230 with a minimal important change of 7 points for the total scale.
Written By Cameron Dyer
References
Drew, B. T., Smith, T. O., Littlewood, C., & Sturrock, B. (2014). Do structural changes (eg, collagen/matrix) explain the response to therapeutic exercises in tendinopathy: a systematic review. British Journal of Sports Medicine, 48(12), 966. doi:10.1136/bjsports-2012-091285
Lemont, H., Ammirati, K. M., & Usen, N. (2003). Plantar fasciitis: a degenerative process (fasciosis) without inflammation. Journal of the American Podiatric Medical Association, 93(3), 234. doi:10.7547/87507315-93-3-234
Lu, H., Gu, G., & Zhu, S. (1996). Heel pain and calcaneal spurs. Zhonghua wai ke za zhi [Chinese journal of surgery], 34(5), 294.
Rathleff, M. S., Molgaard, C. M., Fredberg, U., Kaalund, S., Andersen, K. B., Jensen, T. T., . . . Olesen, J. L. (2015). High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up.(Report). 25(3), e292.
Rathleff, M. S., & Thorborg, K. (2015). ‘Load me up, Scotty’: mechanotherapy for plantar fasciopathy (formerly known as plantar fasciitis). British Journal of Sports Medicine, 49(10), 638. doi:10.1136/bjsports-2014-094562
Riddle, L. D., Pulisic, E. M., Pidcoe, E. P., & Johnson, E. R. (2003). Risk Factors for Plantar Fasciitis: A Matched Case-Control Study. The Journal of Bone & Joint Surgery, 85(5), 872-877. doi:10.2106/00004623-200305000-00015
Taunton, J. E., Ryan, M. B., Clement, D. B., McKenzie, D. C., Lloyd-Smith, D. R., & Zumbo, B. D. (2002). A retrospective case-control analysis of 2002 running injuries. British Journal of Sports Medicine, 36(2), 95. doi:10.1136/bjsm.36.2.95
Thing, J. (2012). Diagnosis and management of plantar fasciitis in primary care. British Journal of General Practice, 62(601), 443-444. doi:10.3399/bjgp12X653769